The big white blobs that look like a baby are the Cysts.
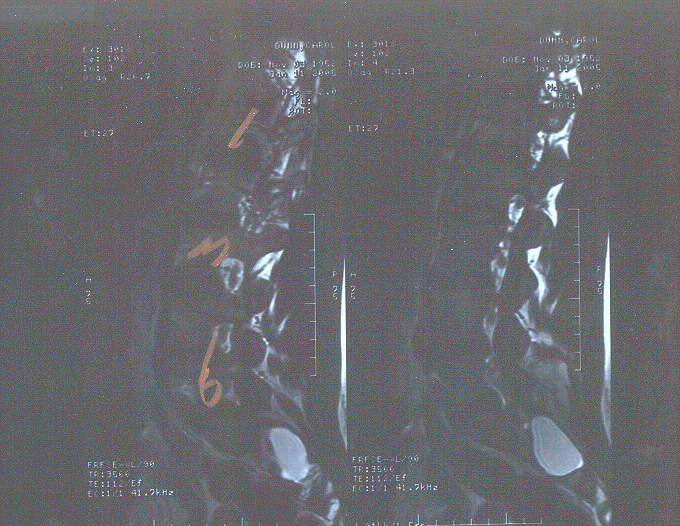
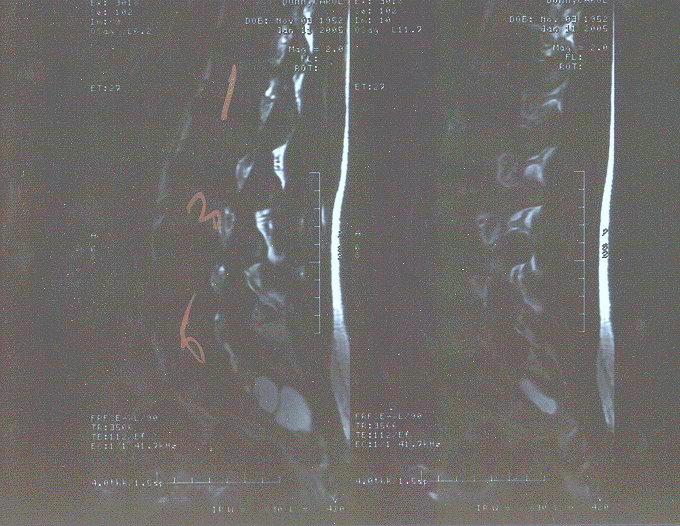
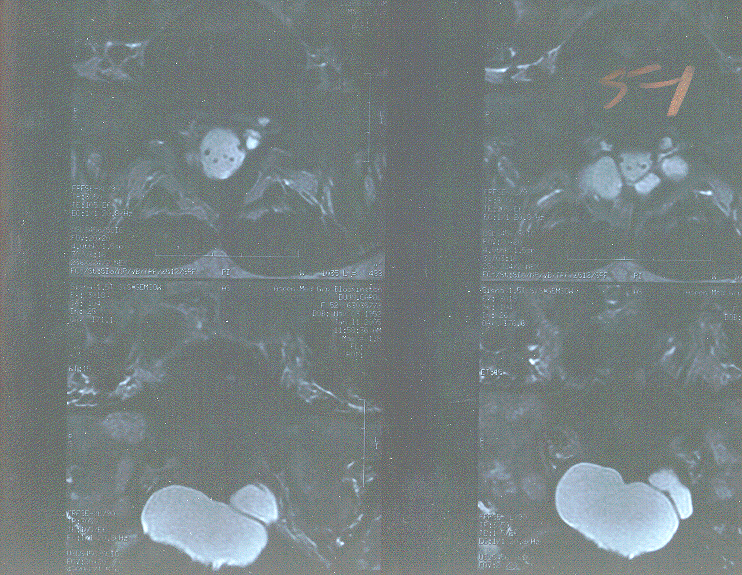
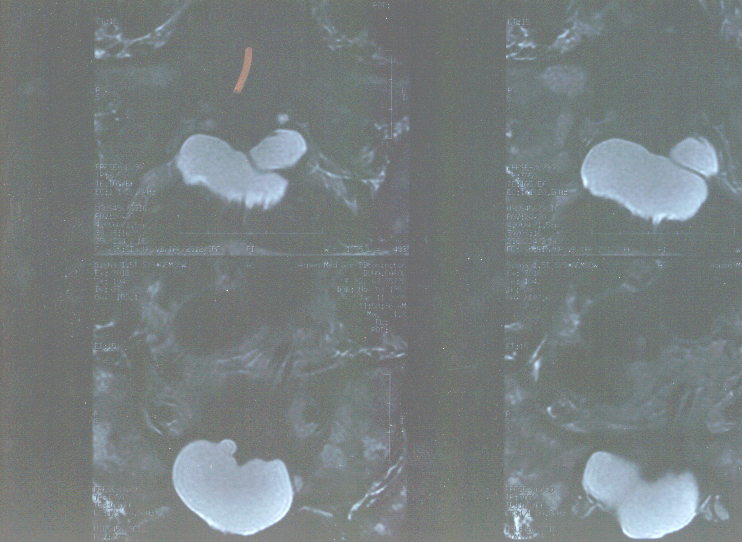
| Aspen Clinic MRI Report by Dr. Irin Weisman 1/11/05 - pertinent info Clinical History: Right leg pain and back pain for six weeks Technical Factors: T1 weighted sagital and axial, T2 weighted sagital and axial. Findings: It is assumed that the patient has five lumbar vertebral bodies. The L4 and L5 disk show mild disk desiccation with no significant disk space narrowing. The lumbar spinal cord terminates posterior to the vertebral body of L1 and a normal-appearing conus medullaris. The vertebral bodies all appear normal. However, in the region of the sacrum, there is a large cystic structure not likely connected to the spinal canal, which appears to be eroding the base of S2. Most likely this represents a Tarlov's cyst. It is primarily on the right side, but also has component that crosses over to the left side. L1-L5 normal. L5-S1: Normal neuroforamina and normal dural sac. However, there is formation of the upper part of the previously described Tarlov's cyst or pseudomeningocele at this level. There does not appear to be any significant impingement on nerve roots by the structures at the level of S1. However, the dominant cyst, which measures approximately 5 x 3 x 5 cm expands into the post-sacral space and occupies the entire volume of the lower sacrum. It appears to erode into the sacrum, but does not appear to impinge on any of the lower sacral nerve roots. There is a left-sided cystic component of this mass, but it appears to be just maximum near the S1 neuroforamen and then decreases in size as the right-sided component expands. The signal characteristics of these lesions are of cerebral spinal fluid. They most likely represent Tarlov's cyst. Facet Joints: The facet joints show minimal degenerative changes at the L4-5 and L5-S1 levels. There is no spondylolisthesis or spondylolysis. Conclusion: Minimal disk degeneration at L4-5 and L5-S1 and large sacral cyst most likely Tarlov's cysts eroding into the sacrum, but without any major spinal nerve root impingement at any level. |
| The Center For Restorative Spine Surgery, 2800 Chicago Ave #402, Mpls MN 55407 Jan 26, 2005 612-879-8084 - the pertinent info from Dr. Charles Burton's report Chief Complaint and Sites of present problem: low back, right anterior thigh pain Present medications: Celebrex and Vicodin. Takes no other medications other than vitamins. Patient is not on anticoagulants and has no known allergies.
Radiology Review: MRI of the lumbar spine from Aspen Medical Group dated 1/11/05 reviewed with patient and husband, Philip. This study shows a underlying diffuse genomic process. It is suspicious for either a lesion or artifact posterior to the body of the L2 vertebra. The study shows that there are large sacral cysts producing erosion of lamina and sacrum, are the Tarlov type. Appearance: Healthy appearing, pleasant, cooperative, well-dressed individual. Good historian. Well oriented as to person, place and time. Displays appropriate mood and affect. No assistive devices. Thoracolumbar Spine: Skin inspection negative for lesions, abnormal pigmentation, asymmetries, or mass lesions. No surgical scars noted. No significant scoliosis or muscle hypertrophy. Range of motion is guarded in all planes. There is 3+ tenderness over right sciatic notch and right popliteal fossa to palpitation with 1+ tenderness over left popliteal fossa and sciatic notch. Diffuse tenderness to palpitation and to percussion over entire lower lumbar and sacral spine. No significant paravertebral spasm. Lower Extremities: Straight Leg Raising: Straight leg raising in the sitting and supine positions is positive on the right to 30 degrees, positive on the left at 70 degrees crossed to the right. Discussion: Ms. Dunn, who is neurologically intact on examination, shows evidence of a right sciatic radiculitis with slight tenderness on the left. Straight leg raising is positive on the right at 30 degrees and crossed from the left. Radiologic studies show large sacral nerve root cysts producing erosion of bone. Ms. Dunn may have some bladder complaints, but that is difficult to be sure of. It is reasonable to assume, but not be certain, that Ms. Dunn's complaints are related to the sacral cysts. Concern is expressed regarding the low resolution of the 1/11/05 MRI. I have recommended a trial of Indocin (75) tablets 1QD to see if the patient's complaints are alleviated. I have recommended that she purchase a sacral pillow (Tush Cush) at the Relax a Back Store in Centennial Lakes. If patient continues to have the complaints noted above, an updated high resolution of the MRI of the lumbar spine will be obtained. Ms. Dunn is a potential candidate for surgical treatment of her sacral cysts. The nature of the procedure, hospitalization and management of this problem have been discussed with patient and her husband. They have also been referred to the website, www.burtonreport.com for additional information. Given the fact that there is a genomic condition, and given the fact that the patient has pain and discomfort in the sitting position, I have provided her with information regarding the Spinal Designs LTX3000 device. |